HR
SV
TPR
VR
SAMPLE PROBLEMS
| HR | SV | TPR | VR | CO | DP | SP | PP | |
| ACh | D | I | D | D | D | D | I | I |
| EPI | I | I | D | I | I | ? | I | I |
| NE | I | I | I | I | I | I | I | I |
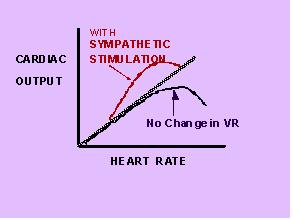
4 Factors Contibuting to Cardiac Output
HR
SV
TPR
VR
As HR increases,Filling Time Decreases!
Digitalis: Decrease HR with no direct
action on contractility or SV
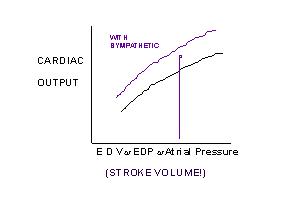
But as filling time increases, EDV increases
so SV increases according to
...
Venous Return: see Fig
13.24
Abdomino-Thorasic (Respiratory) Pump
Skeletal Muscle Pump
Ventricular Diastole
Ventricular Systole
Skeletal Muscle Pump: Fig 13.23
Total Peripheral Resistance
Increased TPR ---> Increased Arterial Pressure
Increases work of heart and length of systole
( esp. isovolumetric phase)
Decrease SV initially and briefly
Also increases Arterial - Venous ![]() P
P
increases amount of blood on venous side
Increase VR and CO?
How do we resolve this apparent conflict/problem?
Depends upon ability of ventricles to increase
SV
Consider exercise......
Response to Light Exercise: Fig 14.12
Blood Pressure
BP expressed in mm Hg
BP = CO x TPR
Pressure measured by baroreceptors
Aortic arch
Carotid sinus
VAGUS NERVE
Parasympathetic fibers
Baroreceptors from aortic arch
Stretch receptors from lungs
Atrial Baroreceptors Responses:Fig 14.1

CHEMORECEPTORS
PO2 receptors
Carotid and aortic bodies
Brain stem - medulla
Sensitive to dissolved O2
Only important at low PO2
Carbonic Anhydrase
CO2 + H2O <--> H2CO3
<--> H+ + HCO3
Lungs
Kidneys
CHEMORECEPTORS: CO2
& pH
AORTIC & CAROTID BODIES
MEDULLA
CO2 + H2O <--> H2CO3
<--> H+ + HCO3-
(AS CO2 INCREASES, PLASMA
& CSF pH DECREASES)
CO2 DISSOLVES FROM PLASMA INTO
CSF ACROSS BLOOD - BRAIN BARRIER
CO2 + H2O <--> H2CO3
<---> H+ + HCO3-
AS PLASMA CO2 INCREASES, PLASMA
pH DECREASES
CO2 DISSOLVES INTO CSF, AND CSF pH DECREASES, STIMULATING MEDULLARY RECEPTORS
INPUTS:
Baroreceptors (pns)
Chemoreceptors (cns & pns)
Atrial volume receptors
Cerebral cortex
Vasovagal syncope (fainting)
Corticohypothalamic response
Flight or fight response
Figure 14.2: Whew !!
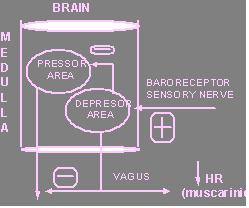
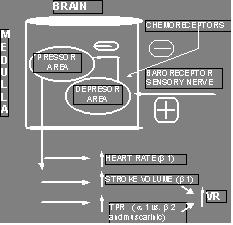
Medullary cardiovascular center
Vasomotor center
Pressor area
Cardioinhibitory center
Depressor area
Pressor or vasomotor center is spontaneously
active and always slowed by depressor which is activated by baroreceptors
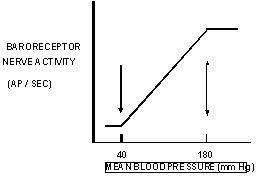
Decreased MAP: Fig 14.3
Increased MAP: Fig 14.3
Receptor-mediated response to hemorrhage:
Fig 14.5
Receptor-mediated response to hemorrhage:
Fig. 14.6
REFLEX RESPONSES
VASOVAGAL SYNCOPE: FAINTING
CORTICOHYPOTHALAMIC DEFENSE REACTION:
FIGHT OR FLIGHT
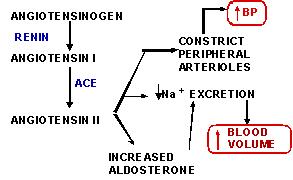
RENAL CONTROL OF BLOOD VOLUME
Mammalian kidneys are designed to reabsorb
Na+ and retain it in body fluids
increase Na+ reabsorption -->increase water
reabsorption -->increase blood volume --->
RAISE BP
ANTIDIURETIC HORMONE:(VASOPRESSIN or ADH)
9 amino acid peptide released from posterior
pituitary
released in response to:
- elevated plasma ![]()
- lowered BP or lowered
blood volume
-(decreased atrial EDV
and/ or decreased baroreceptor distention)
Normally ADH causes Na+ and water reabsorption
by kidneys to increase blood volume and decrease plasma ![]()
ADH released in response to low BP and not
released when BP is high
ATRIAL NATRIURETIC PEPTIDE (ANP)
28 amino acid peptide hormone
released from atrial myocytes (muscle cells)
released in response to distention (high
atrial EDV) due to high BP
INHIBITS Na+ - K+
ATPase in kidney
THUS Na+ AND WATER ARE LOST IN
URINE lowering blood volume
VOLUME RECEPTORS : ATRIAL STRETCH RECEPTORS:
DECREASE ADH
And
INCREASE ANP (increase urine
output and decrease blood volume)
ATRIAL STRETCH RECEPTORS RESPOND TO INCREASED BV BY:
RENIN -ANGIOTENSIN - ALDOSTERONE
LOW RENAL BLOOD FLOW
(< 20% OF CO) ---> ACTIVATION OF
POTENT VASOCONSTRICTOR:
ANGIOTENSIN
Things to Review and Know !
Table 14.1
Fig 14.7