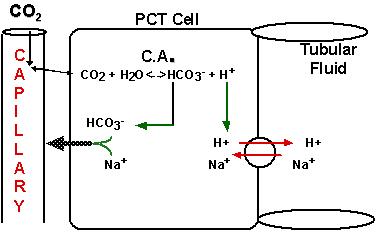
Active transport of Na+, glucose, amino acids, and phosphate (HPO4-2 & H2PO4-)
Water and Cl- usually follow the charge and osmotic gradients
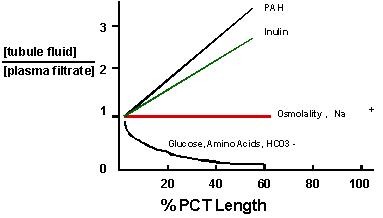
Reabsorption in PCT: Fig 17.13 & Fig 17.14
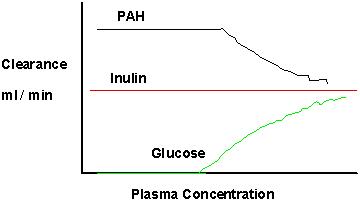
Secretion / Reabsorption: Fig 17.19
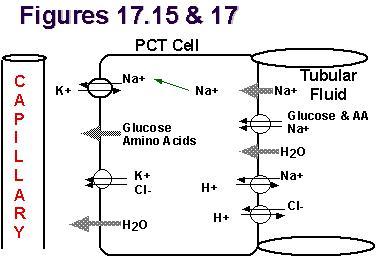
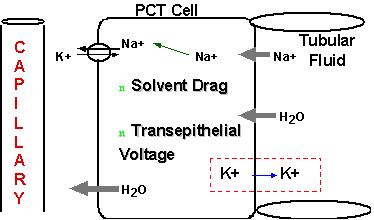
Reabsorption in the PCT : Fig 17.15
Active transport of Na+, glucose, amino acids, and phosphate (HPO4-2
& H2PO4-)
Water and Cl- usually follow the charge and osmotic gradients
Reabsorption:
Active, therefore specificity and saturation
Amino acids --> neutral, acidic, and basic sites
Tmax (tubular maximum)
Energy from ion gradients (co-transport or symport) or ATP
Reabsorption in PCT:
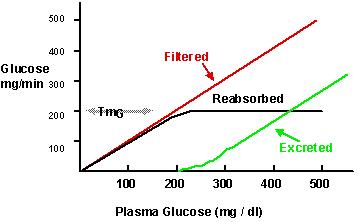
As with any transport system, saturation occurs at high [plasma]solute
, giving a maximum rate of reabsorption or a Tmax for each reabsorbed
solute.
Tmax depends upon # of transport sites
Reabsorption in PCT: Fig 17.16
Na+ Reabsorption in PCT: Fig 17.17
Na+ Reabsorption in DCT: Fig 17.17
Cell-Cell Junctions in CTs: Fig 17.18
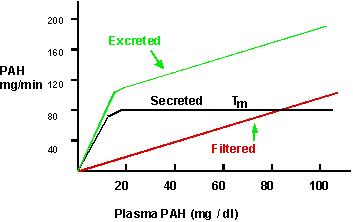
PCT & DCT Secretion
Organic Anions
Phenol Red
PAH
Creatinine
Penicillin
Acetazolamide
Furosemide
PCT & DCT Secretion
Organic Cations
Histamine
Norepinephrine
Quinine
Creatinine
QUESTION:
If secretion is a carrier mediated process, how does one explain the
presence of transport sites for solutes not found in nature?
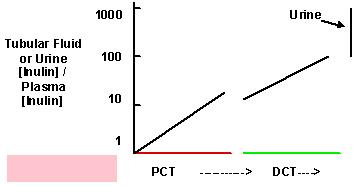
[Solute]nephron
Blood = 300 mOsm
Bowmans Capsule = 285 mOsm
PCT = 285 mOsm
Loop of Henle = 285 ---> 1,200 ---> 200 mOsm
DCT = 200 ---> 100 ---> 200 mOsm
CD = 200 ---> 285 ---> variable to 1,200 mOsm - [ADH] dependent