Salivary Glands
Ģ Parotid
Ģ Submaxillary & Sublingual
mucin (protein for lubrication)
Salivary Glands: Fig 19.9
Salivary Glands
Ģ Parotid
![]() amylase (ptyalin)
amylase (ptyalin)
![]() 1 - 4 hexose linkages
1 - 4 hexose linkages
Ģ Submaxillary & Sublingual
mucin (protein for lubrication)
Salivary Glands - Acinus type glands:
Primary secretion by secretory cells and then modified by duct cells
as saliva passes through on the way to the oral cavity
Accessory Gland Structure: Fig 19.8
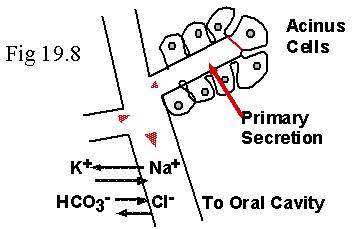
Saliva
As saliva flows down duct: [Na+] and [Cl-] decrease,
[HCO3-] and [K+] increase
(![]() also decreases)
also decreases)
As flow rates increase, this exchange is less complete
Salivary pH
Saliva pH is basic (vs. plasma pH)
WHY?? (i.e., for what purpose?)
Excitatory Signal Molecules
ACh from Parasympathetic NS onto muscarinic receptors
VIP from enteric NS
Increased blood flow in response to kininogen activation
Kininogen Activation
Ģ Glands release Kallikrein when activated
Ģ Plasma globulin
Ģ Results in peptide --> bradykinin
Ģ Bradykinin ---> local vasodilation (10X increase in BF)
Other Components of Saliva
Ģ Muramidase --> cleave muramic acid in bacterial cell walls
Ģ Lactoferrin --> binds Fe++
Ģ Epidermal growth factor --> stimulates mucosal cell growth
Ģ IgA
Ģ Lingual lipase (small amounts)
Ģ ABO antigens (secreters)
Salivary Secretion
Ģ Cephalic Phase
Thought or sensory input
Ģ Gastric Phase
Distention
Secretagogues
Vagal - Vagal reflex
Peristalsis
Requires only enteric n.s. for short distances
Enhanced by parasympathetic excitation
duration, velocity, amplitude all increased
Reflex relaxation ensures oral --> anal direction & sphincter opening
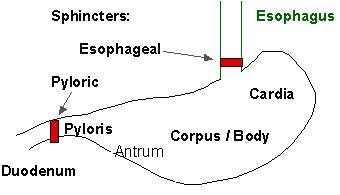
Stomach; Figure 19.4
Stomach Mucosal Surface: Folds are called Rugae gastricae
Achalasia: failure to open esophageal sphincter
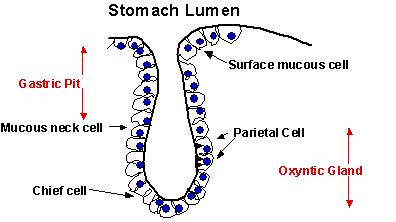
Gastric Glands
Ģ Cardiac
mucous producing columnar cells
Ģ Pyloric
mucous and G cells producing peptide hormone gastrin
Ģ Oxyntic; Oxyntic Glands
Ģ Surface Epithelium - insoluble mucous
Ģ Neck Cells - soluble mucous
Ģ G cells - gastrin
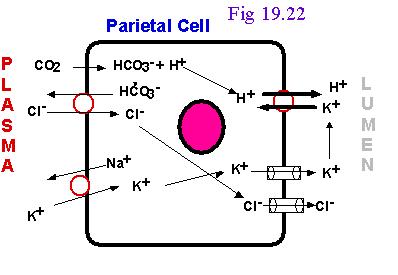
Ģ Parietal (or oxyntic) Cells - HCl & Intrinsic Factor
Ģ Chief Cells - pepsinogen
Ģ D cells - enterogastrones
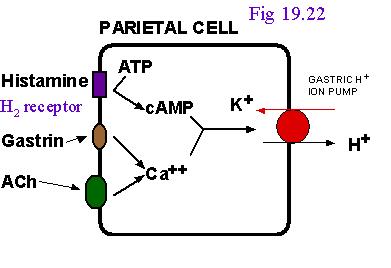
Gastric Acid Secretion: Fig 19.22
Histamine
From enterochromafin-like cells (ECL cells) in the gastric mucosa
Ģ produce, store, & release histamine
Ģ activated by ACh, gastrin, & secretagogues
Postprandial Alkaline Tide
Treatment of Hyperacidity
Ģ Atropine
Ģ Cimetidine
Ģ Antihistamine (H2 antagonists)
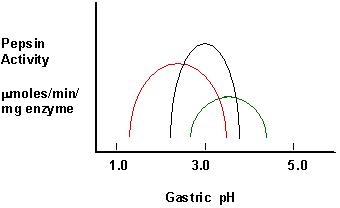
Pepsin
Ģ Pepsinogen ---> pepsin in acidic conditions of stomach
Ģ It is a family of endopeptidases
Ģ pH optima 1.8 - 3.5
Ģ Activation of Pepsin; Fig 19.14
Intrinsic Factor
Ģ binds Vitamin B12
Ģ protects it from gastric and intestinal digestion
Ģ absorbed as IF-Vit B12 complex in ileum by receptor mediated
endocytosis
Ģ absence = pernicious anemia
Secretagogues
Ģ caffeine and theophylline
Ģ peptides
Ģ spices
Ģ Alcohol
Ģ aspirin
Table 19.2 Gastrointestinal Hormones
Contol of G.I. Function: Fig. 19.21
GASTRIN
Ģ Peptide hormoneFrom G cells
Ģ Increases HCL & pepsinogen secretion
Ģ Increases gastric motility and emptying into duodenum
Gastric Acid Secretion:
Cephalic Phase Fig 19.23a
Ģ Thought of food, smell, chewing, swallowing
Ģ Vagus nerve to parietal cells (ACh)
Ģ Vagus nerve (ACh) onto G cells & thus causes gastrin release
Ģ See TABLE 19.2 !!!!!
Gastric Phase Fi 19.23b
Ģ Stomach distention & peptides
Ģ Local (enteric) reflexes & vagovagal reflexes to
Ģ Parietal cells (ACh)
Ģ G cells (release gastrin)
Ģ Gastric Acid Secretion:
Intestinal Phase
Ģ Stimulus - digested peptides, peptides in duodenum, distention
Ģ G cells (gastrin)
Ģ distention -->Intestinal endocrine cells release enterooxyntin
Inhibition of Gastric Secretion
Ģ Important for protection of duodenum
Ģ Gastric pH < 3 ---> gastric D cells release somatostatin (?) which
inhibits gastrin release
Ģ Acid in duodenum ---> secretin & CCK---> inhibits gastric secretion
and motility
Ģ Acid, fats, hyper-osmotic solutions in the duodenum ---> release
of enterogastrones --->
inhibit gastric motility and secretion
Ģ Gastric Inhibitory Peptide (GIP) from duodenum ---> inhibits parietal
cell function
Ģ Inhibitors of Gastric Secretion
Ģ GIP
Ģ CCK
Ģ Secretin
Ģ See Table 19.2
Ulcers: Peptic & Duodenal
Role of Helicobacter pylori
Vomit reflex
Note sympathetic symptoms
Fig 19.10: The Pancreas
Fig 19.11a: Liver
Fig 19.11b: Liver
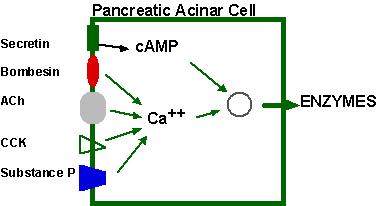
Cholecystokinin (CCK) & Secretin
Both hormones produced in duodenum in response to chyme content
Hormone receptors in pancreatic cells
Pancreatic Secretions:
Hydrelatic
Ģ HCO3- rich aqueous fluid
Ģ neutralizes stomach HCl
Ģ dilutes the chyme
Ecbolic
Ģ enzyme rich secretion
Ģ Proteases - endopeptidases
Ģ Trypsinogen ---> trypsin
Ģ Chymotrypsinogen --> chymotrypsin
Ģ Proelastase --> elastase
Ģ Proteases - exopeptidases
Ģ Procarboxypeptidase --> carboxypeptidase
Ģ Proaminopeptidase --> aminopeptidase
Ģ amylase
Ģ Lipases
Ģ Ribonuclease
Ģ Deoxyribonuclease
Protease Activation
Ģ Pancreatic secretion contains trypsinogen and trypsin inhibitor
Ģ Enterokinase in intestine activates trypsin
Ģ Trypsin inhibitor is diluted by chyme
Hormonal Regulation of Pancreatic Secretion
Ģ Secretin
peptide hormone
pancreatic secretion rich in HCO3-
Ģ Cholecystokinin (CCK)
peptide hormone (33 amino acids)
pancreatic secretion rich in enzyme
Pancreatic Secretion:
Ģ Cephalic Phase
Sight, taste, smell of food
Release of ACh & gastrin in response to vagal stimulation
Increased pancreatic flow, especially ecbolic
Ģ Gastric Phase
Protein in chyme --> gastrin
Gastric distention --> ACh from vagus
Increased pancreatic secretion, esp. ecbolic
Ģ Intestinal Phase
Acid in chyme --> secretin
hydrelatic secretion
Long chain fatty acids & amino acids and peptides in chyme
CCK & vagovagal reflex
ecbolic secretion
Bile from the Liver
Bile Acids
Primary from cholesterol by addition of OH and COOH
Secondary formed in intestine by resident bacteria
conjugated to taurine or glycine
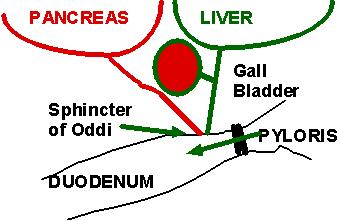
Bile Flow
Released as CCK causes contraction of gall bladder and relxation of
Sphincter of Oddi
CCK (33 amino acid hormone) released in response to fatty acids and
lipids in chyme
Gall Bladder Storage of Bile
Gall Bladder stores bile and removes Na+ and water.
Thus bile may be concentrated as much as 20X
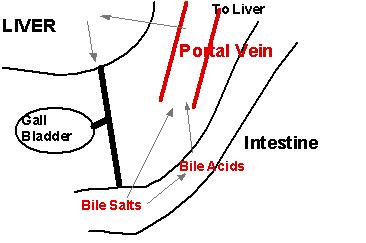
Recirculation and reuse of bile salts and acids
Bile salts and acids are reabsorbed from intestine (ileum) into portal
blood
From portal blood, liver reabsorbs bile salts and acids and reconjugates
them for reuse
Bile Flow
As portal blood bile salts and acids increases, bile synthesis decreases
Thus one has bile-dependent and bile-independent flow